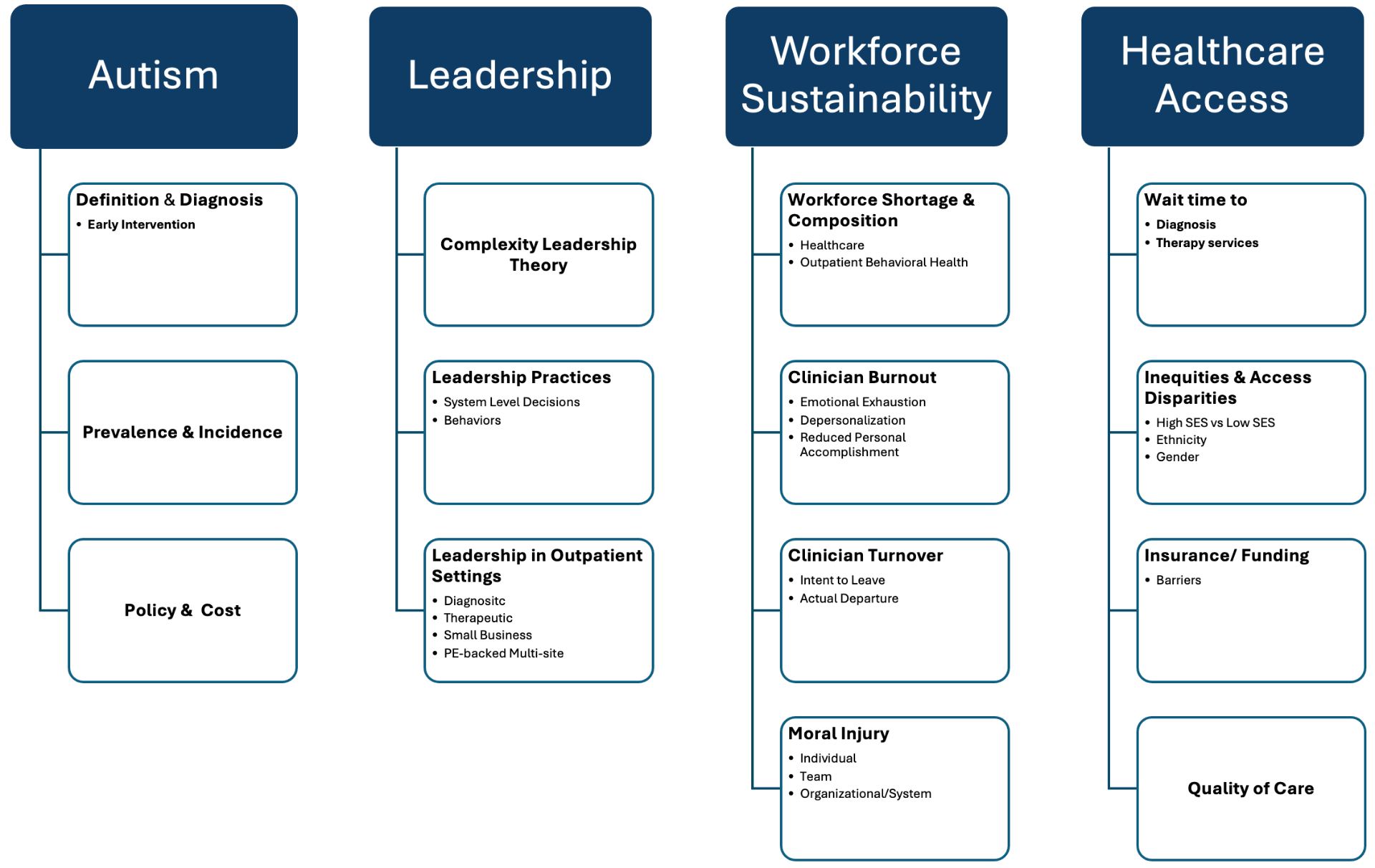
Domain 1Autism
The population at the center of the question.
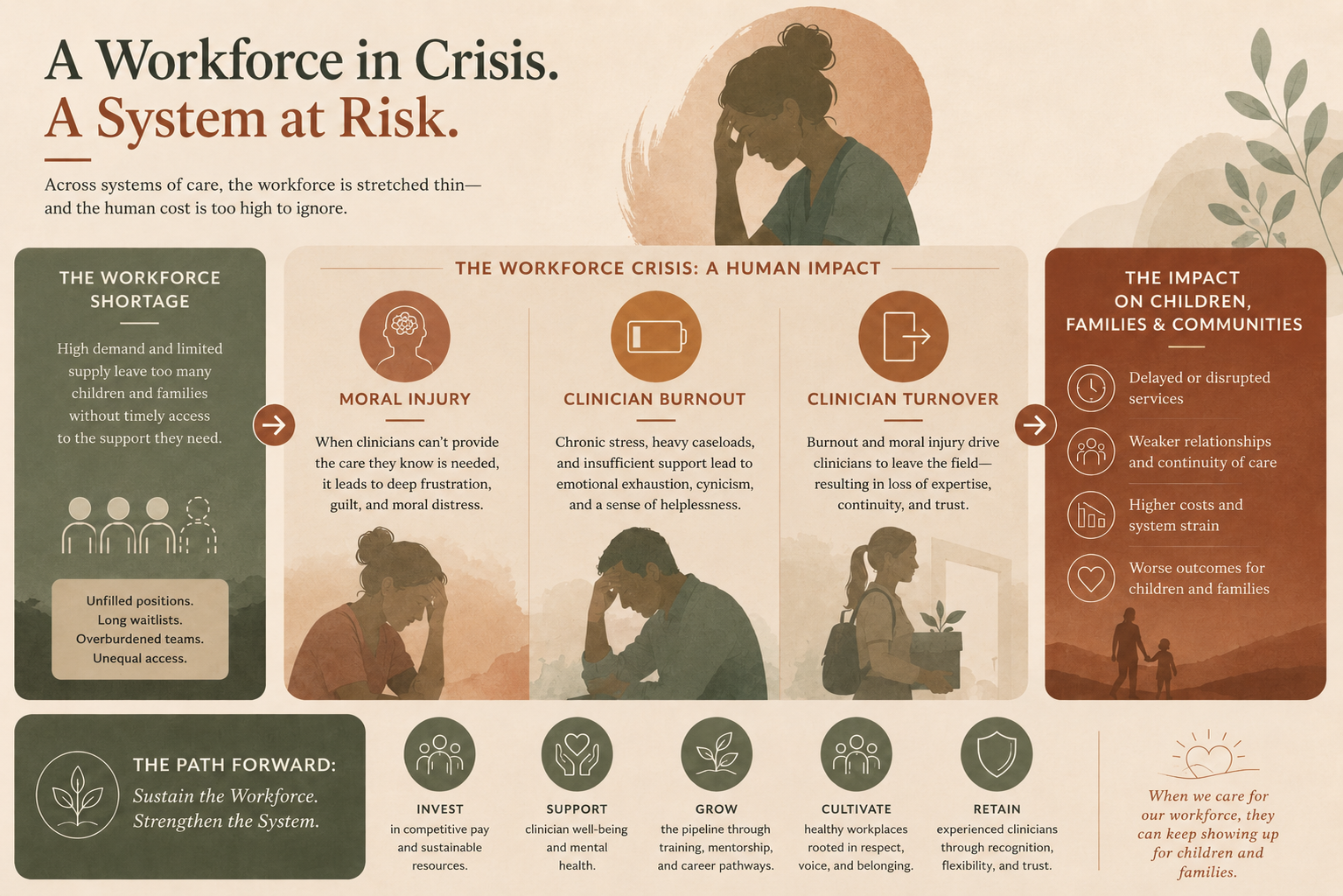
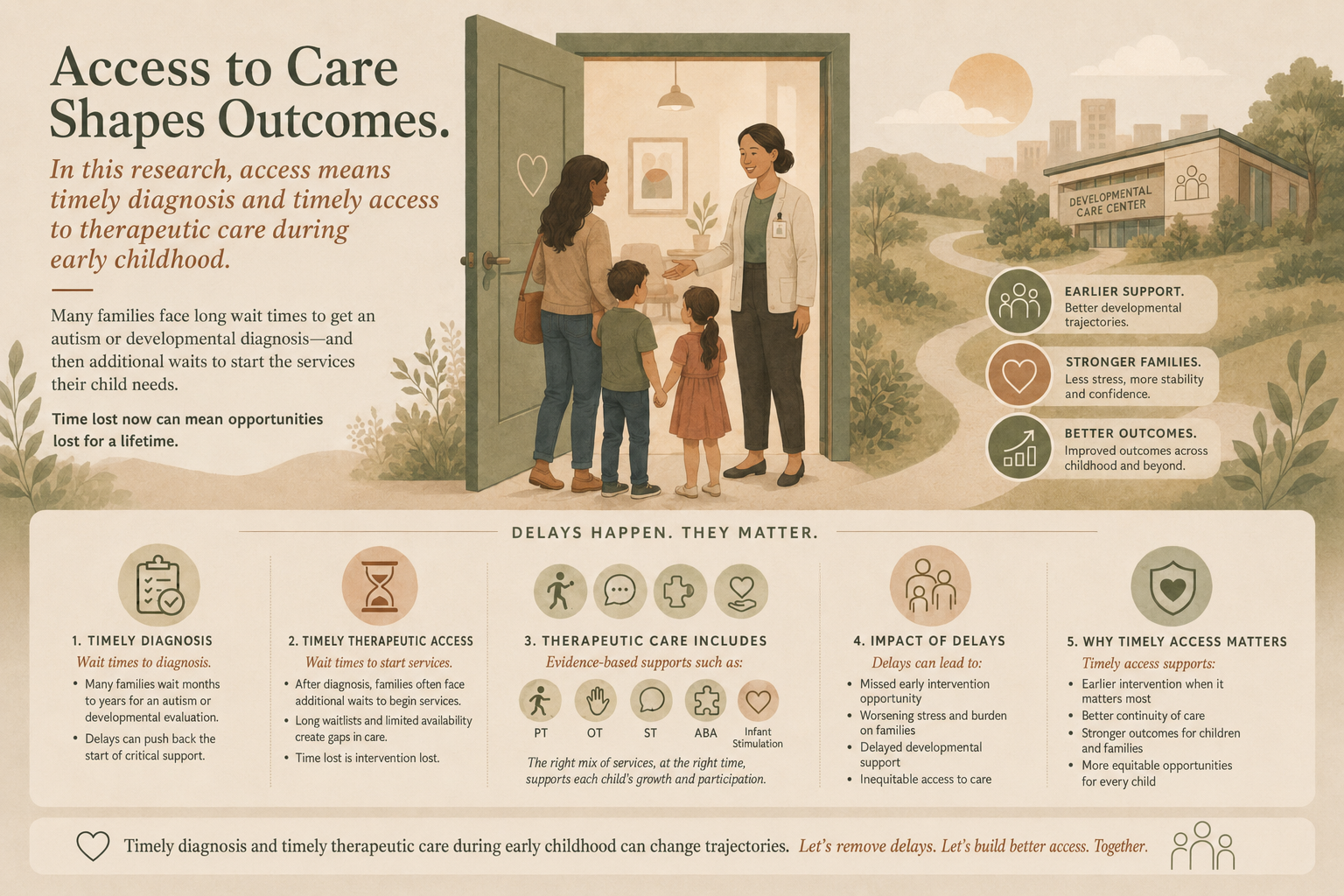
ASD remains one of the top neurodevelopmental and most disabling disorders among children, with the first published case reported in 1943 (Isaac et al., 2025; Talantseva et al., 2023). Autism prevalence has risen from 1 in 150 children in 2002 to 1 in 31 in 2022. In American children with developmental delays, 12% under the age of three experience delays in access to care, and 90% are not identified at the youngest age possible (Scherr et al., 2020). Demand for diagnostic and therapeutic services has outpaced outpatient capacity.
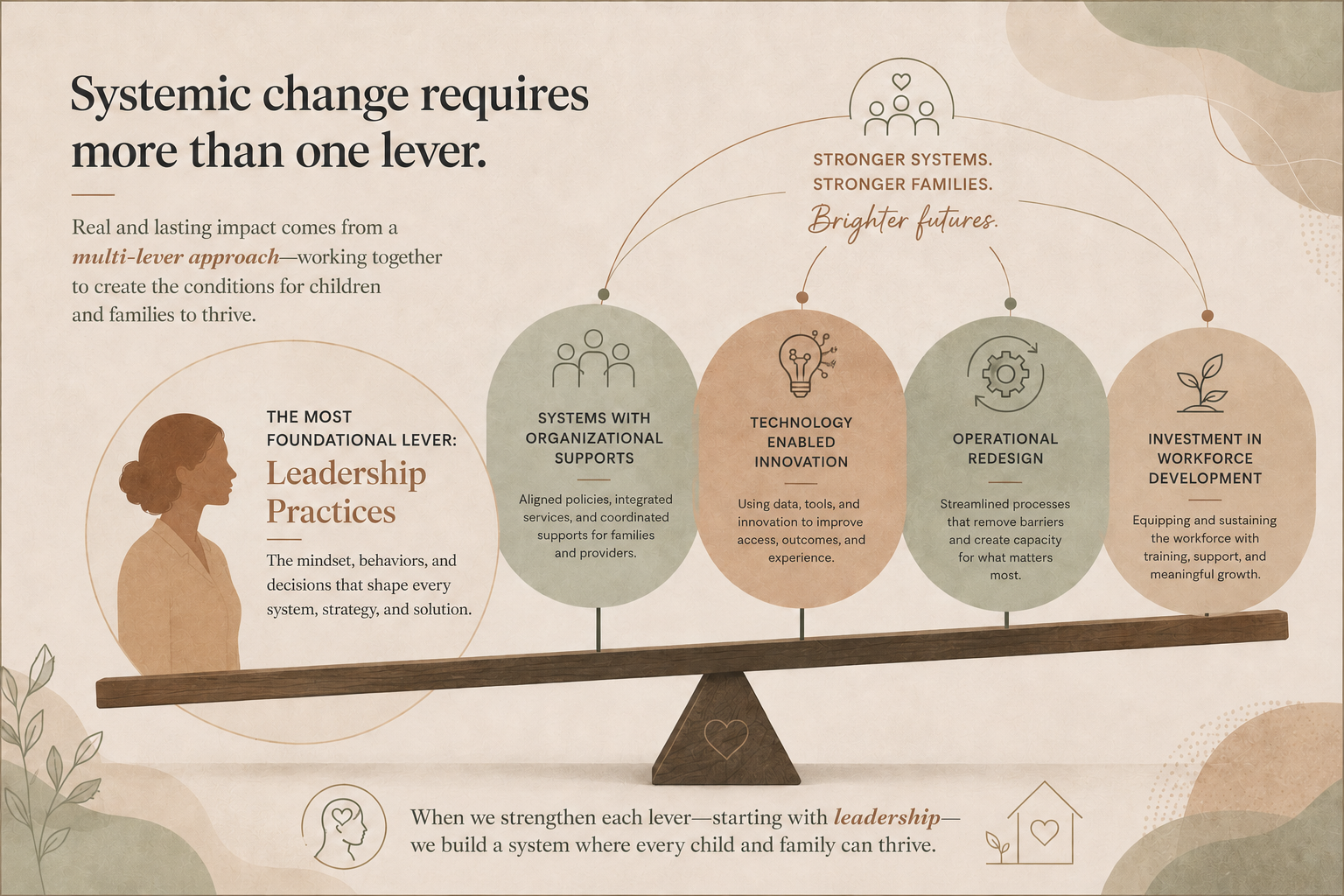
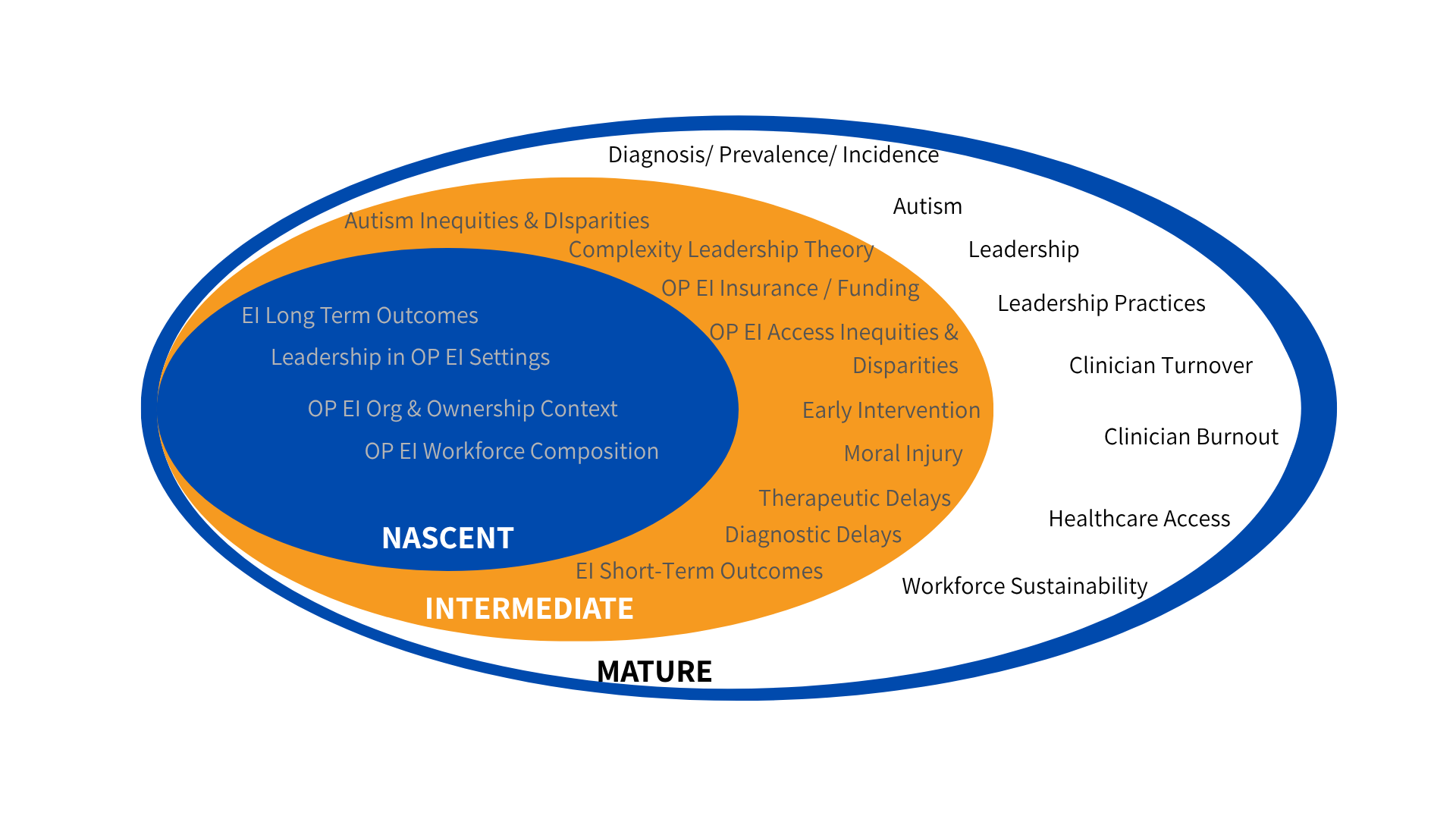
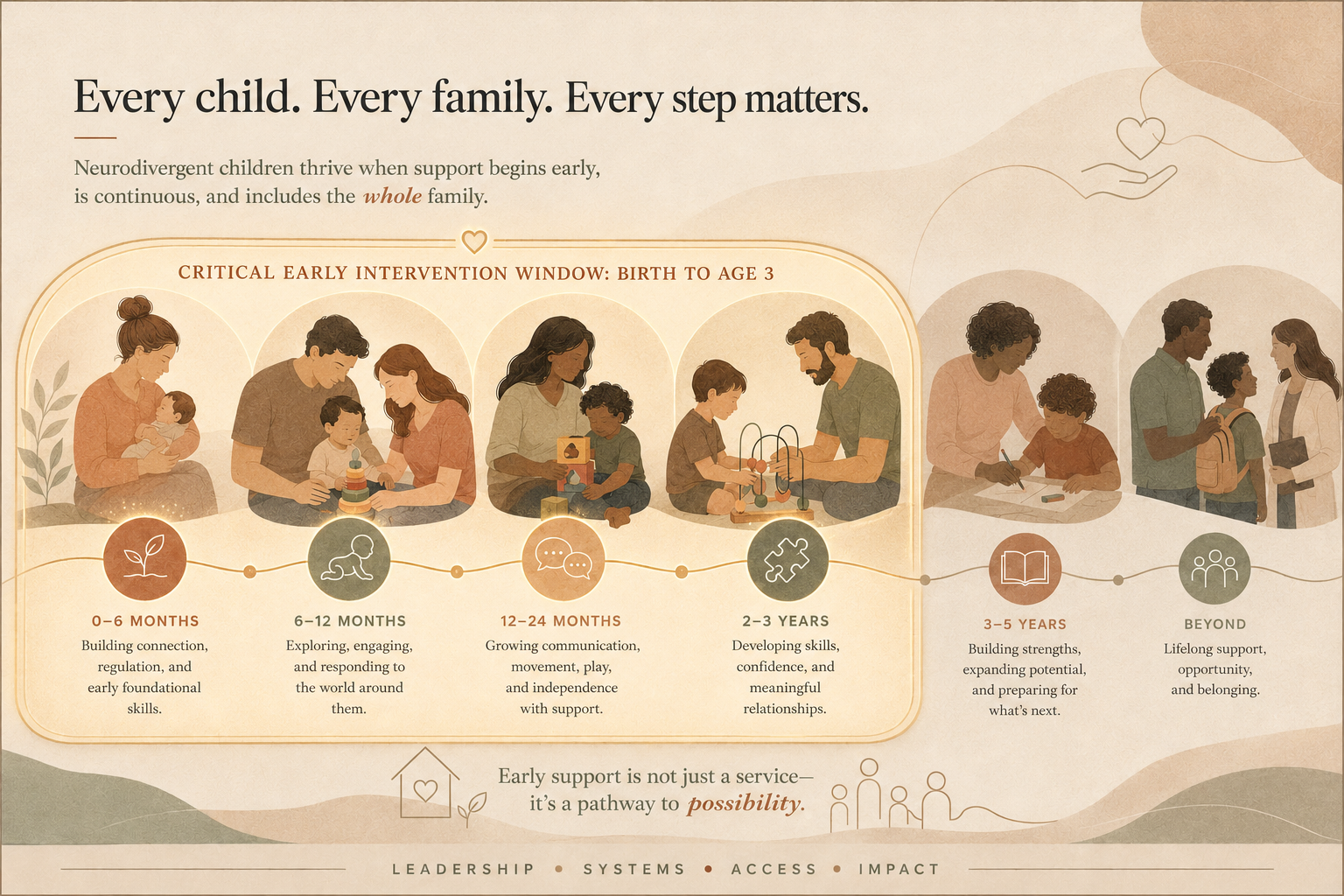
The literature is mature on definition and diagnosis, prevalence and incidence, and policy and cost, and increasingly clear that the early intervention window is where outcomes are made or missed.
DEFINITION & DIAGNOSISPREVALENCEPOLICY & COSTEARLY INTERVENTION